
ブログ
認知症の治療薬、使い分けについて、名古屋市千種区の児童精神科医が解説
認知症の治療薬、使い分けについて、名古屋市千種区の児童精神科医が解説
こんにちは、名古屋市千種区 児童精神科専門クリニック、医療法人永朋会 和光医院、加藤晃司です。
今回は、認知症の治療薬、使い分けについて解説します。
認知症の治療薬は、原因疾患や症状のタイプによって適切に使い分ける必要がある非常に専門的な領域です。以下に、アルツハイマー型認知症(AD)を中心に、レビー小体型(DLB)や血管性認知症(VaD)なども含めた治療薬の使い分けを、最新の知見と臨床実践に基づいて詳細に解説します。
【1】認知症治療薬の基本分類(2025年時点で国内使用可能)
◆ 認知機能を改善・維持する薬(いわゆる「抗認知症薬」)
ドネペジル(アリセプト)
ガランタミン(レミニール)
リバスチグミン(リバスタッチ、イクセロンパッチ)
メマンチン(メマリー)
◆ 行動・心理症状(BPSD)への対症薬(適応外使用含む)
抗精神病薬(クエチアピン、リスペリドンなど)
抗うつ薬(SSRI、ミルタザピンなど)
抗てんかん薬(バルプロ酸など)
【2】タイプ別の薬剤の使い分け
① アルツハイマー型認知症(AD)
最も多いタイプで、アセチルコリンの枯渇が認知症の主な原因の一つとされています。
治療の第一選択は**コリンエステラーゼ阻害薬(ChE-I)**です。
◆ 初期〜中等度
ドネペジル:最も歴史が長く、汎用性が高い
ガランタミン:ニコチン受容体を介した作用もあり、注意力や集中の改善が期待される
リバスチグミン:貼付薬があり、嚥下困難や服薬コンプライアンス不良の患者にも対応可
◆ 中等度〜高度
メマンチン:NMDA受容体拮抗薬。興奮毒性を抑制し、過活動や攻撃性にも効果あり
ドネペジル+メマンチンの併用も中等度以降では選択肢となる
② レビー小体型認知症(DLB)
幻視やパーキンソニズム、自律神経症状が目立つタイプ。薬物過敏性があり、慎重な投与が必要。
第一選択:ドネペジル(幻視の軽減にも効果あり)
メマンチンは使用されるが過鎮静や幻覚の悪化に注意
抗精神病薬は最小限で使用、非定型薬を低用量で使用(クエチアピンなど)
③ 血管性認知症(VaD)
脳血管障害に伴う認知機能低下で、明確な治療薬はありませんが、コリンエステラーゼ阻害薬が補助的に使われることもあります。
ドネペジルの有効例が一部にあり(とくにAD合併例)
血圧、脂質、糖尿病の管理が中心
抑うつや意欲低下が強ければ、**ミルタザピンやドパミン活性を補う薬(メチルフェニデートなど)**が使われることも
④ 前頭側頭型認知症(FTD)
感情コントロール障害、常同行動、脱抑制が中心。コリンエステラーゼ阻害薬は効果が乏しいか、逆に行動障害を悪化させることも。
原則として抗認知症薬は推奨されない
行動障害に対して抗精神病薬や抗うつ薬の少量使用
【3】薬剤別の特徴と選び方のポイント
◉ ドネペジル(アリセプト)
作用:コリンエステラーゼ阻害(脳内アセチルコリンを増加)
用量調整しやすく、ADにもDLBにも使える汎用性
副作用:悪心・下痢・食欲低下(特に開始初期に注意)
◉ ガランタミン(レミニール)
作用:コリンエステラーゼ阻害+ニコチン受容体作動性
注意力・覚醒度が比較的改善しやすい
注意点:夜間の中途覚醒や不眠を訴えることがある
◉ リバスチグミン(リバスタッチ・イクセロンパッチ)
作用:中枢型・末梢型両方のChEを阻害(貼付剤)
パッチ型のため、服薬が難しい患者に有効
注意点:皮膚刺激(かぶれ)や体臭の変化に注意
◉ メマンチン(メマリー)
作用:NMDA受容体拮抗 → 興奮毒性を抑制
特に攻撃性・落ち着きのなさ・BPSDに有効
高齢・腎機能低下の患者には慎重投与
【4】BPSD(行動・心理症状)への対処薬
認知機能よりも、**「怒りっぽい」「幻覚」「徘徊」「不眠」などの行動症状(BPSD)**が強い場合、抗認知症薬だけでは限界があるため、以下の薬が使われることがあります(すべて適応外使用)。
クエチアピン:幻視・妄想への第一選択(DLBでも比較的安全)
リスペリドン:短期的な攻撃性に有効(ただし脳卒中リスク増加に注意)
ミルタザピン:食欲低下、抑うつ、不眠を同時に改善しやすい
バルプロ酸:興奮・不穏のコントロール(エビデンスは限定的)
【5】使い分けの実践的アルゴリズム(概要)
認知症のタイプを特定(AD/DLB/VaD/FTD)
中核症状(記憶障害など)が中心 → 抗認知症薬で改善を狙う
行動症状(怒り・幻視・興奮)が中心 → 抗精神薬・抗うつ薬を併用
吐き気・体重減少・かぶれなどの副作用を見ながら個別調整
【6】まとめ
抗認知症薬は「どれか1つが優れている」のではなく、「病型と症状に応じて適切に選ぶ」ことが重要です。
認知機能を補う治療は早期介入がより効果的とされており、進行後はBPSD対策とのバランス調整が鍵になります。
過鎮静や副作用のリスクを避けつつ、QOLを保つことがゴールです。
当院ホームページはこちらより
ご予約は公式ライン、ホームページから可能です。
友達追加はこちらから↓
当院インスタグラムはこちら
https://www.instagram.com/wako_iin/
子どものためのメンタルクリニック
医療法人永朋会 和光医院
児童精神科・精神科・心療内科
〒464-0092 愛知県名古屋市千種区茶屋が坂1丁目12番2号
電話 : 052-712-1777
地下鉄名城線「茶屋ヶ坂」駅 1番出口より徒歩3分
地下鉄名城線「砂田橋」駅 1番出口より徒歩10分
Dementia Treatment: How to Choose the Right Medication
Explained by Dr. Koji Kato, Child Psychiatrist at Wako Clinic, Chikusa Ward, Nagoya City
Hello, I’m Dr. Koji Kato, a child psychiatrist at Wako Clinic, a specialist mental health clinic in Chikusa Ward, Nagoya City.
Today, I will explain how dementia medications are selected and differentiated.
Dementia medications must be chosen appropriately depending on the underlying cause and the nature of the symptoms. Below is a detailed explanation based on current medical knowledge and clinical practice, focusing primarily on Alzheimer’s disease (AD), but also including dementia with Lewy bodies (DLB) and vascular dementia (VaD).
[1] Classification of Dementia Medications (Available in Japan as of 2025)
◉ Drugs that improve or maintain cognitive function (“anti-dementia drugs”)
Donepezil (Aricept)
Galantamine (Reminyl)
Rivastigmine (Rivastach, Exelon Patch)
Memantine (Memary)
◉ Drugs for behavioral and psychological symptoms of dementia (BPSD)
Often used off-label
Antipsychotics (e.g., quetiapine, risperidone)
Antidepressants (e.g., SSRIs, mirtazapine)
Anticonvulsants (e.g., valproic acid)
[2] Choosing Medication by Dementia Type
① Alzheimer’s Disease (AD)
The most common type. Cholinergic neuron degeneration is central, so cholinesterase inhibitors (ChE-Is) are the first-line treatment.
Mild to moderate stage:
Donepezil: Most widely used, flexible dosing.
Galantamine: Also works via nicotinic receptors—may help improve attention.
Rivastigmine: Available as a patch—helpful for patients with swallowing difficulties or poor adherence.
Moderate to severe stage:
Memantine: NMDA receptor antagonist. Helps with agitation and hyperactivity.
Combination of Donepezil + Memantine is often used at this stage.
② Dementia with Lewy Bodies (DLB)
Characterized by hallucinations, parkinsonism, and autonomic dysfunction. Patients are often sensitive to medications.
First choice: Donepezil (shown to reduce hallucinations)
Memantine is used cautiously—can cause over-sedation or worsen hallucinations.
Antipsychotics must be used minimally and very cautiously (e.g., low-dose quetiapine).
③ Vascular Dementia (VaD)
Caused by cerebrovascular events. No definitive drugs, but ChE-Is may be used in mixed AD/VaD cases.
Donepezil may help in some cases.
Primary focus is on managing vascular risk factors: hypertension, dyslipidemia, diabetes.
If apathy or depression is prominent, mirtazapine or dopaminergic agents (e.g., methylphenidate) may be considered.
④ Frontotemporal Dementia (FTD)
Marked by emotional dysregulation, disinhibition, and stereotyped behavior. ChE-Is are generally ineffective and may worsen symptoms.
Anti-dementia drugs are generally not recommended.
Low-dose antipsychotics or antidepressants are used to manage behavioral symptoms.
[3] Drug Characteristics and Selection Tips
◉ Donepezil (Aricept)
Increases brain acetylcholine by inhibiting cholinesterase.
Versatile—can be used in both AD and DLB.
Side effects: Nausea, diarrhea, appetite loss (especially early on).
◉ Galantamine (Reminyl)
Dual action: cholinesterase inhibition + nicotinic receptor modulation.
May improve alertness and focus.
Side effects: May cause insomnia or night-time awakenings.
◉ Rivastigmine (Rivastach / Exelon Patch)
Inhibits both central and peripheral cholinesterase.
Patch form is good for patients with swallowing issues or poor medication adherence.
Side effects: Skin irritation, body odor changes.
◉ Memantine (Memary)
NMDA receptor antagonist—reduces excitotoxicity.
Especially useful for agitation, aggression, or BPSD.
Use with caution in elderly or those with renal impairment.
[4] Medications for BPSD (Behavioral and Psychological Symptoms of Dementia)
When behavioral symptoms (e.g., aggression, hallucinations, wandering, insomnia) are more problematic than cognitive decline, anti-dementia drugs alone are often insufficient. Off-label medications are used, such as:
Quetiapine: First choice for hallucinations and delusions—relatively safe in DLB.
Risperidone: Effective for acute aggression—but carries a risk of stroke.
Mirtazapine: Improves appetite, mood, and sleep—useful for patients with depression and weight loss.
Valproic acid: May help with agitation or irritability—evidence is limited.
[5] Practical Algorithm for Medication Selection
Identify the type of dementia: AD / DLB / VaD / FTD
If cognitive symptoms dominate → use anti-dementia drugs
If behavioral symptoms dominate → add antipsychotics or antidepressants
Monitor for side effects like nausea, weight loss, skin issues
Adjust the regimen based on tolerability and patient/family goals
✅ Conclusion
There is no “one best medication” for dementia. The key is personalized selection based on dementia type, symptom profile, and patient characteristics.
Early intervention is more effective for cognitive preservation, while later stages require careful balancing of behavioral symptoms and safety.
The ultimate goal is to preserve quality of life (QOL) while minimizing side effects and maintaining patient dignity.
受診される方へ
初めて受診される方
当院は予約制をとっておりますが、初診の場合は若干のお時間をいただくこととなり、お待ちいただくことがあります。スムーズにご案内する為に、WEB問診のご利用をおすすめいたします。
WEB問診はこちら >
初診予約は電話にてお願いします。
再診される方
お電話もしくは予約システム(チェック・オン)から予約を取ることもできます。予約の変更や取り消しをご希望の場合には、診療時間内に受付にお電話いただくか、予約システムから変更・取り消しを行ってください。
パソコン・携帯から簡単にご予約できます。
和光医院 診療時間のご案内
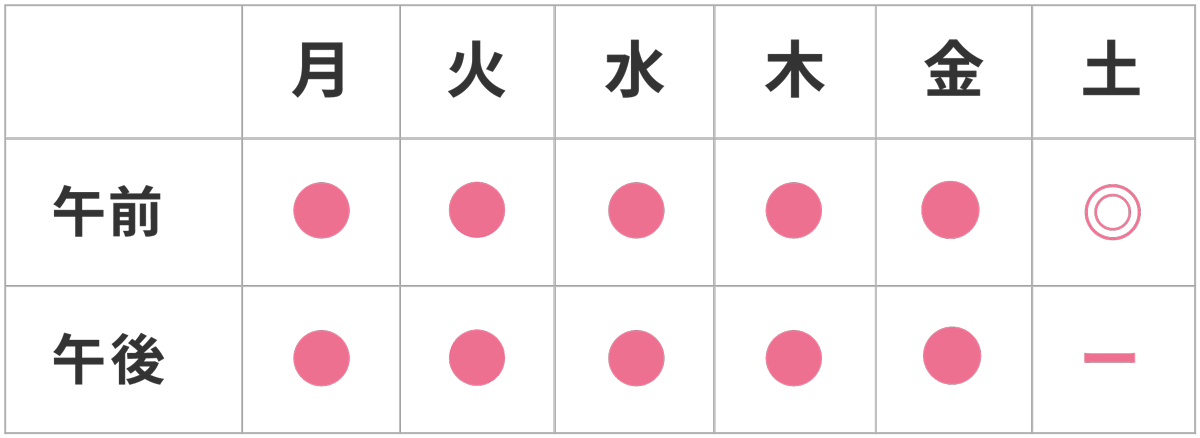
【診療時間】
午前 9:00〜13:00
午後 15:00〜18:00
土曜 9:00〜14:00
【休診日】 日・祝日
患者様へのご案内
- 明細書について:当院では、療養費規則に基づき明細書の発行を無料で行っています。
- 一般名による処方について:後発医薬品が存在する場合は、商品名ではなく一般名(有効成分名)で処方することがあります。
- 医療情報の活用について:当院では、安心な医療を提供する為、オンライン資格確認や電子処方箋データ等の情報を活用して診療を行っています。